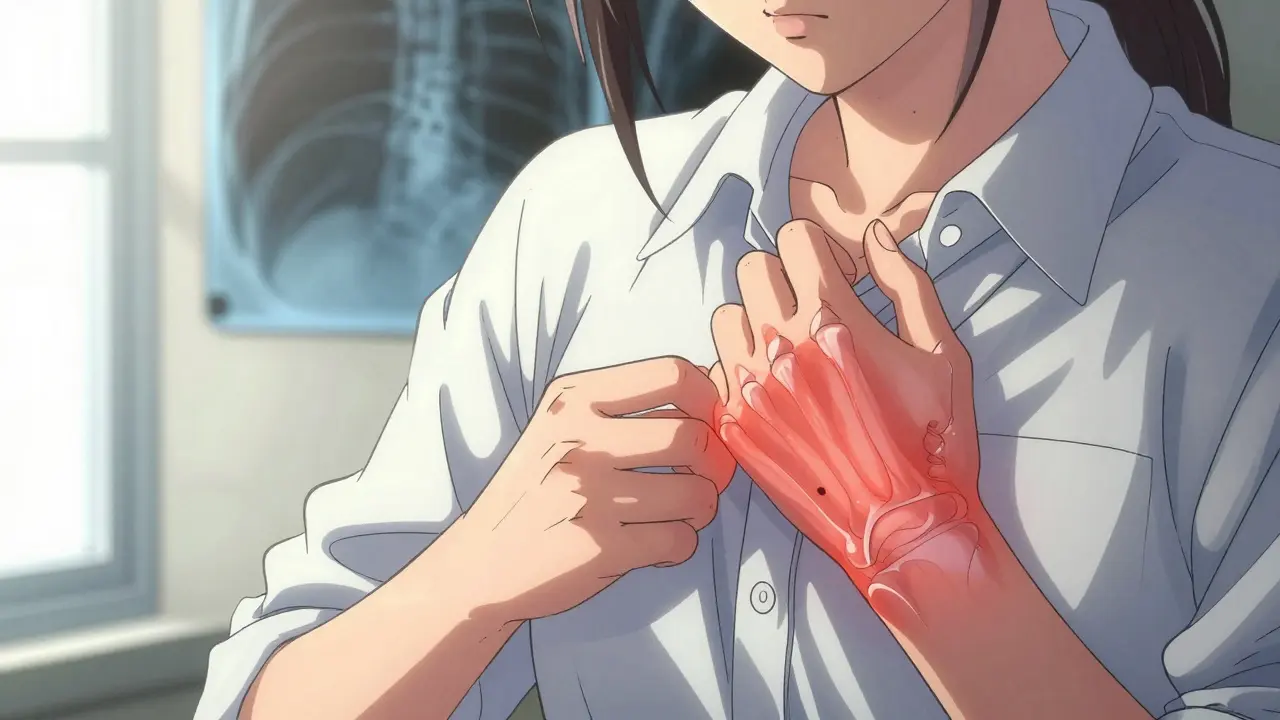
When your hands swell up in the morning and even buttoning a shirt feels impossible, it’s not just aging-it could be rheumatoid arthritis (RA). Unlike the wear-and-tear kind of joint pain from osteoarthritis, RA is an autoimmune disease where your body turns on itself. Your immune system, meant to protect you, starts attacking the lining of your joints. This triggers inflammation, pain, stiffness, and over time, permanent damage. It doesn’t just affect joints. It can hit your lungs, heart, eyes, and even lower your red blood cell count. And it’s not rare: about 1.3 million Americans live with it, with women two to three times more likely to be diagnosed than men.
How Rheumatoid Arthritis Really Works
RA doesn’t show up overnight. It creeps in. You might notice a dull ache in your knuckles, stiffness that lasts longer than 30 minutes after waking, or swelling in both wrists at the same time. That symmetry is a red flag-RA typically hits matching joints on both sides of the body. The culprit? The synovium, the thin tissue lining your joints that normally makes fluid to keep them moving smoothly. When your immune system attacks it, the synovium thickens, swells, and starts destroying cartilage and bone. X-rays show it clearly: early on, there’s soft tissue swelling; later, the space between bones shrinks, and tiny holes appear in the bone near the joint.
Genetics play a role. Variations in HLA genes, especially HLA-DR4, increase risk. But genes alone don’t cause RA. Something has to trigger it-like a viral infection, smoking, or even long-term exposure to silica dust. That’s why two people with the same genetic risk can have very different outcomes. About 10-15% of people with RA also develop Sjögren’s syndrome, where the immune system attacks tear and saliva glands, leaving eyes dry and mouth parched. And beyond the joints, RA raises your risk of heart disease, lung scarring, and even certain lymphomas.
Diagnosis: More Than Just Pain
There’s no single test for RA. Doctors use a mix of clues. Blood tests look for rheumatoid factor (RF) and anti-CCP antibodies. While not everyone with RA tests positive, anti-CCP is more specific-if it’s high, the chance of developing severe joint damage is much greater. Imaging matters too. Ultrasounds can spot inflammation before X-rays show damage. MRI scans reveal early bone changes that X-rays miss. The American College of Rheumatology’s diagnostic criteria require at least six weeks of joint symptoms, morning stiffness lasting over 30 minutes, and involvement of multiple joints. If you’ve had swelling in three or more joints for over six weeks, especially in the hands or feet, it’s time to see a rheumatologist.
One big mistake? Waiting. Too many people think, “It’ll pass,” or “I’m just tired.” But the window to prevent permanent damage is narrow-within the first 3 to 6 months after symptoms start. After that, joint erosion becomes harder to stop. That’s why early diagnosis isn’t just helpful-it’s critical.
First-Line Treatment: Methotrexate and Why It Still Matters
Before biologics, methotrexate was the only real option. Today, it’s still the foundation. Why? It works. It’s cheap. And it’s effective for about 60-70% of patients. Methotrexate is a DMARD-disease-modifying antirheumatic drug-that slows down the immune system broadly. It doesn’t cure RA, but it can stop or slow joint damage. Most patients start with methotrexate alone, often at a weekly dose of 15-25 mg. Side effects? Nausea, fatigue, liver stress. But with folic acid supplements and regular blood tests, most manage it well.
Here’s the catch: if methotrexate doesn’t bring your disease activity down to low or remission levels within 3-6 months, you need to move up. That’s where biologics come in. The European League Against Rheumatism (EULAR) and American College of Rheumatology both recommend adding a biologic if targets aren’t met by that 6-month mark. Delaying means more damage.
Biologic Therapies: Targeted Weapons Against RA
Biologics are made from living cells, not chemicals. They target very specific parts of the immune system that drive inflammation in RA. Unlike methotrexate, which acts like a shotgun, biologics are sniper rifles. The first one approved was etanercept in 1998. Since then, several classes have emerged:
- TNF inhibitors: Adalimumab (Humira), etanercept (Enbrel), infliximab (Remicade). These block tumor necrosis factor, a key inflammatory protein. They’re the most prescribed biologics-about 55% of all biologic use.
- IL-6 inhibitors: Tocilizumab (Actemra). Blocks interleukin-6, a signal that tells immune cells to attack joints. It’s especially helpful for patients with high inflammation markers.
- B-cell inhibitors: Rituximab (Rituxan). Depletes B-cells, which produce the antibodies that attack joints.
- T-cell costimulation blockers: Abatacept (Orencia). Stops T-cells from getting activated in the first place.
Combining a biologic with methotrexate boosts effectiveness. Clinical trials show that about 60% of patients on a biologic plus methotrexate cut their disease activity by 50% or more. Alone, methotrexate gets you to that level in 40%. That difference matters-less pain, fewer flares, and better function.
Real people see results. Sarah K., 42, stopped playing piano for five years because her fingers were too stiff and deformed. After starting tocilizumab in 2022, she could hold a pen again-and eventually, she returned to the keyboard. Stories like hers aren’t rare. The Arthritis Foundation’s patient survey found 65% of biologic users regained ability to do daily tasks.
The Cost and Risk Trade-Off
But biologics aren’t magic. They come with serious downsides. First, cost. Annual treatment can run $15,000 to $60,000. Even with insurance, copays can hit $500 a month. That’s why 41% of patients say cost blocks consistent use. The first biosimilar to adalimumab (adalimumab-adaz) was approved in September 2023. It’s expected to cut prices by 15-20%-a small but real relief.
Second, risk. Biologics suppress your immune system. That means higher chances of serious infections-tuberculosis, pneumonia, even fungal infections. Studies show a 1.5 to 2 times higher risk than with methotrexate alone. That’s why the FDA requires all biologics to have a Risk Evaluation and Mitigation Strategy (REMS). Before starting, you get tested for TB. You’re told to avoid live vaccines. If you develop a fever that won’t go away, you stop the drug and call your doctor.
Long-term, there’s a small but real risk of lymphoma. It’s rare-about 1 extra case per 1,000 patients over 10 years-but it’s real. That’s why doctors weigh risks carefully. A 25-year-old with aggressive RA? The benefit outweighs the risk. A 70-year-old with mild symptoms and heart disease? Maybe not.
What Comes Next: JAK Inhibitors and the Future
Biologics aren’t the only option anymore. JAK inhibitors like upadacitinib (Rinvoq) and tofacitinib (Xeljanz) are oral pills that block the same inflammatory pathways, but inside cells instead of outside. They’re faster-acting than biologics and don’t need injections. Rinvoq got expanded approval for early RA in January 2024. They’re now used in about 15% of cases.
Research is moving fast. Scientists are looking for biomarkers-genetic or blood markers-that can predict who will respond to which drug. One study using genetic data predicted methotrexate response with 85% accuracy. That’s huge. Imagine a simple blood test telling you: “This drug will work for you. This one won’t.” That’s the future.
Drugs in phase 3 trials include selective TYK2 inhibitors like deucravacitinib. These are more targeted than JAK inhibitors, with fewer side effects. They could hit the market between 2025 and 2027.
Living With RA: Beyond Medication
Medication is only part of the story. You also need movement. The CDC recommends 150 minutes of moderate exercise a week-walking, swimming, cycling. Exercise doesn’t worsen RA; it helps. It keeps joints flexible, muscles strong, and reduces pain. Losing 5-10% of body weight can cut disease activity by 20-30% in overweight patients.
Stress management matters too. Chronic stress can trigger flares. Mindfulness, yoga, or even just 10 minutes of deep breathing daily can help. And don’t ignore sleep. Poor sleep makes pain worse and inflammation higher.
Support is critical. The Arthritis Foundation’s Live Yes! Network has 100,000 members. Online communities like Reddit’s r/rheumatoidarthritis (with 28,500 members) offer real advice: how to open jars with one hand, which shoes to buy, how to talk to your boss about fatigue. These aren’t just forums-they’re lifelines.
What to Do If You Suspect RA
If you’ve had joint pain, swelling, or stiffness for more than six weeks-especially in small joints and worse in the morning-don’t wait. See your doctor. Ask for RF and anti-CCP blood tests. Request an ultrasound if swelling is still there. Don’t accept “it’s just arthritis.” Push for a rheumatology referral. Early treatment saves joints. Delaying treatment by even three months increases your risk of permanent damage.
And if you’re already diagnosed? Track your symptoms. Use apps like MyRA (downloaded over 250,000 times). Log pain levels, fatigue, stiffness, and medication side effects. Bring it to every appointment. Ask: “Am I in remission? If not, what’s the next step?”
RA isn’t a death sentence. But it demands action. The tools exist. The science is clear. The goal isn’t just to feel better-it’s to stay independent, active, and in control of your life. And with the right treatment, that’s absolutely possible.
Can rheumatoid arthritis be cured?
No, there is no cure for rheumatoid arthritis yet. But with early and aggressive treatment, many people achieve remission-meaning no signs of active disease. In remission, joint damage stops, pain disappears, and daily function returns. The goal of modern RA care isn’t just to manage symptoms-it’s to reach and maintain remission.
Are biologics safe for long-term use?
Biologics are generally safe for long-term use when monitored closely. The biggest risks are serious infections and a small increase in lymphoma risk. Regular blood tests, TB screening, and avoiding live vaccines reduce those risks. Most patients stay on biologics for years, especially if they’re working. The benefits of preventing joint destruction and disability usually outweigh the risks.
Why do some people stop taking biologics?
The top reasons are cost, side effects, and lack of access. About 30% of patients stop biologics within the first year. High out-of-pocket costs are the biggest barrier, cited by 52% of patients. Others quit due to infections, injection site reactions, or because they didn’t feel better. Some patients also don’t get regular follow-ups and don’t realize their dose might need adjustment.
Do biologics work better than methotrexate alone?
Yes, for many people. When used together, biologics and methotrexate are significantly more effective than methotrexate alone. Clinical trials show that 60% of patients on combination therapy cut their disease activity by 50% or more, compared to 40% with methotrexate alone. The combination also slows joint damage better and increases the chance of achieving remission.
Can lifestyle changes replace medication for RA?
No. Lifestyle changes like diet, exercise, and weight loss can reduce symptoms and improve response to medication-but they cannot replace disease-modifying drugs like methotrexate or biologics. RA is an autoimmune disease that attacks joints. Only medications that target the immune system can stop the damage. Lifestyle changes support treatment; they don’t substitute for it.





Comments (11)
Ray Foret Jr.
I was diagnosed with RA last year and honestly? This post saved my life. I thought I was just getting old. Now I'm on methotrexate and it's changed everything. Still tired sometimes, but I can hold my kid again. 💙
Scott Easterling
Yeah right... biologics? You think Big Pharma really cares about your joints? They're just milking you for $60k/year while you go broke. I've seen people on Humira get fungal infections that never went away. And don't get me started on the lymphoma stats... they bury that in fine print. Someone's got to wake up.
Samantha Fierro
Thank you for writing this with such clarity. I'm a nurse and I've watched too many patients delay care because they thought it was 'just stiffness.' Early intervention isn't optional-it's everything. If you're reading this and hesitating, please, call your rheumatologist today. You deserve to live fully.
Robert Bliss
I've been on Orencia for 3 years. It's not perfect but I can finally tie my shoes again. Also, walking my dog used to make me cry. Now? We go 3 miles. Small wins count. 🙏
Peter Kovac
The data presented here is statistically incomplete. The 60% efficacy rate for combination therapy is cherry-picked from phase III trials with strict inclusion criteria. Real-world effectiveness drops to 38% due to non-adherence, comorbidities, and pharmacokinetic variability. This post is dangerously optimistic.
APRIL HARRINGTON
I cried reading this I mean like full on ugly crying because I thought I'd never play guitar again and now I'm doing little riffs and my fingers dont feel like broken glass anymore I just want everyone to know you are not alone
Leon Hallal
They don't tell you the truth. Biologics are just a Band-Aid on a bullet wound. You think your body's not still attacking itself? You're just numbing the signal. I've been on three different ones. I'm tired of being a lab rat. And the cost? It's a prison.
Judith Manzano
I love how this breaks down the science without dumbing it down. I'm a grad student in immunology and I wish more public health content was this accurate. Also-yes to exercise! I started swimming and my CRP levels dropped 40% in 4 months. It's not magic, but it's medicine too.
rafeq khlo
Methotrexate is poison. They say it's cheap but they don't say it's slowly killing your liver. I know a guy who got cirrhosis at 38. And now they push biologics like they're candy. Wake up. This system is rigged.
Philip Mattawashish
You're all being manipulated. The real cause of RA? Glyphosate. The same chemical in Roundup that's in your bread, your beer, your tap water. The pharmaceutical industry doesn't want you to know because they profit from treating symptoms, not eliminating the root. Glyphosate disrupts your gut microbiome → autoimmune cascade. Stop taking their drugs. Go organic. Or keep paying.
Morgan Dodgen
The TNF-alpha blockade paradigm is fundamentally flawed. It's a reductionist approach in a complex cytokine network. You suppress TNF, IL-6 rises. Suppress IL-6, GM-CSF explodes. The field needs systems biology, not shotgun immunosuppression. And don't get me started on JAK inhibitors-JAK1/2/3 inhibition is a genomic sledgehammer. We're treating symptoms with molecular carpet bombing. Pathetic.