Imagine your skin slowly losing its elasticity, becoming tight and hard, while the internal organs you rely on every second begin to stiffen. This is the reality for people living with Scleroderma is a chronic autoimmune disease where the body produces too much collagen, leading to the thickening and hardening of the skin and connective tissues. Also known as systemic sclerosis, it doesn't just affect the surface; it can penetrate deep into the lungs, heart, and digestive system, making a simple task like swallowing food or taking a deep breath a daily struggle.
What Exactly Is Scleroderma?
At its core, this condition is a glitch in the immune system. Instead of protecting the body, the immune system attacks the connective tissue. This triggers an overproduction of collagen-the protein that gives your skin structure. When too much collagen builds up, tissues lose their stretch. According to the American College of Rheumatology, this rare condition affects about 300 per million people globally. Interestingly, it predominantly hits women, with a 4:1 female-to-male ratio, usually appearing between the ages of 30 and 50.
Doctors generally split the disease into two main camps. First, there is localized scleroderma, or morphea, which is essentially a skin-deep issue. It causes hard patches of skin but doesn't mess with your internal organs. Then there is systemic scleroderma, the more aggressive version that can impact multiple organ systems. If you have the systemic version, your internal organs are at risk: about 90% of patients experience gastrointestinal issues, and 80% deal with lung complications.
Spotting the Warning Signs
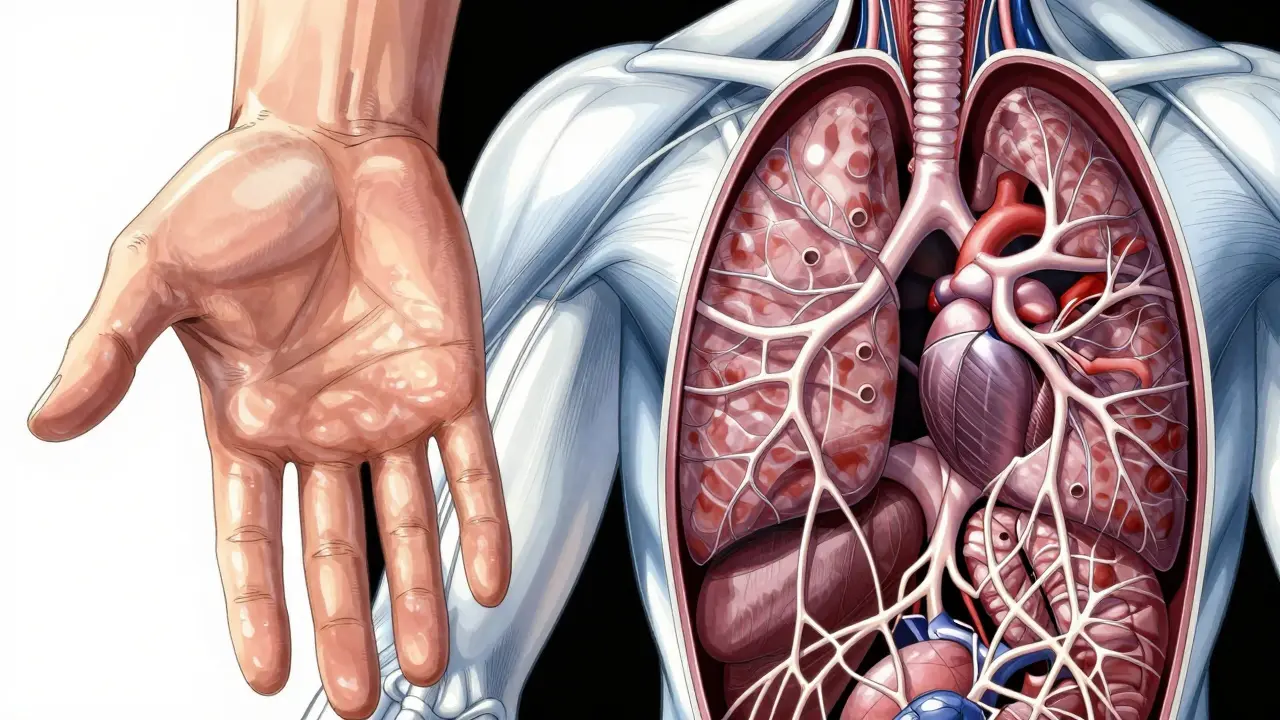
Scleroderma rarely arrives with a clear announcement. Instead, it creeps in with subtle symptoms that people often ignore or misdiagnose. The most famous early warning is Raynaud's phenomenon, where fingers turn white or blue when exposed to cold or stress. In about 90% of systemic cases, this happens 5 to 10 years before any other symptoms appear. If your fingers are changing colors frequently, it's a signal that the blood vessels are struggling.
Another hallmark is sclerodactyly, which is the thickening and tightening of the skin on the fingers. This makes the hands look shiny and prevents them from flexing fully. Because these early signs are so nonspecific, many patients end up in a "diagnostic odyssey," seeing an average of 3.2 different doctors over 18 months before someone finally gives them the correct diagnosis.
The Different Pathways of Progression
Not every patient follows the same path. The disease is often categorized by how quickly it moves and how much of the body it affects. We call these the limited and diffuse versions.
Those with limited cutaneous systemic sclerosis usually see a slower progression over 10 to 20 years. Their skin thickening is typically restricted to the hands, face, and feet. On the other hand, people with diffuse cutaneous systemic sclerosis experience rapid skin thickening across the trunk and limbs within the first 3 to 5 years. This group faces a higher risk of early internal organ failure.
| Feature | Limited Cutaneous | Diffuse Cutaneous |
|---|---|---|
| Skin Involvement | Hands, face, feet (Limited) | Trunk and limbs (Widespread) |
| Progression Speed | Slow (10-20 years) | Rapid (3-5 years) |
| 10-Year Survival | 75-85% | 55-70% |
| Primary Risk | Pulmonary Hypertension | Pulmonary Fibrosis |

The Role of Antibodies in Diagnosis
Since the symptoms overlap with other diseases, doctors rely heavily on blood tests to find specific antibodies. These markers don't just confirm the disease; they help predict how it will behave. For instance, if a patient tests positive for anti-Scl-70 (Topoisomerase I) antibodies, they are much more likely to develop pulmonary fibrosis, a scarring of the lung tissue that makes breathing difficult.
In contrast, anti-centromere antibodies (ACA) are common in the limited version of the disease. These patients usually have a lower risk of severe organ involvement but a higher chance of developing pulmonary arterial hypertension. There are also anti-RNA polymerase III antibodies, which often signal a more rapid progression of skin thickening and a higher risk of cancer.
How Scleroderma Differs from Other Autoimmune Diseases
It's easy to confuse scleroderma with lupus or rheumatoid arthritis because they all involve the immune system attacking the body. However, the "mechanism of injury" is different. In rheumatoid arthritis, the joints swell because of inflammation. In scleroderma, the joints often stiffen because the skin around them has turned into a rigid shell-this is called a contracture.
While Lupus is more common, affecting millions, scleroderma is rarer but more focused on fibrosis. The "perfect storm" of this disease is the combination of autoimmunity, vasculopathy (blood vessel damage), and fibrosis (scarring). This triple threat is what makes it so devastating to organ function compared to diseases that are primarily inflammatory.

Managing the Daily Struggle
Living with this condition requires more than just a once-a-month checkup with a general practitioner. Because the disease hits so many different systems, a multidisciplinary team is essential. You need a rheumatologist to lead the way, but you'll likely also need a pulmonologist for your lungs, a cardiologist for your heart, and a gastroenterologist for the digestive tract.
Treatment is a challenge because there are very few FDA-approved drugs specifically for scleroderma. Many doctors repurpose medications from other autoimmune conditions. For example, Tocilizumab was a major milestone as the first drug approved specifically for scleroderma-associated interstitial lung disease. Other management strategies include:
- Skin Care: Using thick moisturizers and avoiding triggers that cause Raynaud's episodes.
- GI Support: Managing severe reflux and swallowing difficulties through diet and medication.
- Wound Care: Treating digital ulcers on the fingertips, which can require multiple weekly visits to a specialist.
- Lung Monitoring: Annual high-resolution CT scans and pulmonary function tests to catch fibrosis early.
Many patients also use adaptive devices. Since hand contractures make it hard to button clothes or open jars, tools like button hooks and electric jar openers become essential for maintaining independence.
Looking Ahead: New Hope and Research
The future of scleroderma care is moving toward more targeted therapies. Researchers are currently testing B-cell depletion therapies and tyrosine kinase inhibitors to stop the scarring process before it becomes permanent. One of the most exciting developments is the SCOT trial, which looked at autologous hematopoietic stem cell transplantation. In some cases, this showed a 50% improvement in skin scores after 54 months.
We're also seeing the rise of telemedicine. Programs like the one at Stanford have shown that virtual visits can reduce hospitalizations by 32% for rural patients. This is critical because specialized centers of excellence are rare-only about 35% of U.S. patients have access to one. As we find better ways to manage the disease, we are seeing an aging population of survivors, which brings new challenges in managing the disease alongside old-age health issues.
What is the difference between localized and systemic scleroderma?
Localized scleroderma (morphea) only affects the skin, causing hardened patches without involving internal organs. Systemic scleroderma affects the skin and can damage internal organs like the lungs, heart, and kidneys, making it a much more serious condition.
Is scleroderma curable?
Currently, there is no known cure for scleroderma. However, treatment focuses on managing symptoms, preventing complications (like lung scarring), and improving the quality of life through medications and physical therapy.
Why are Raynaud's symptoms important?
Raynaud's phenomenon, where fingers change color in the cold, is often the very first sign of systemic scleroderma. It can appear 5 to 10 years before skin thickening or organ involvement, providing a critical window for early diagnosis.
Which organs are most commonly affected by systemic sclerosis?
The gastrointestinal tract is affected in about 90% of cases, followed by the lungs (80%), the heart (30-45%), and the kidneys (10-15%). Pulmonary arterial hypertension and pulmonary fibrosis are the most significant threats to survival.
What are the most common blood tests for scleroderma?
Doctors look for Antinuclear Antibodies (ANA), which are positive in 95% of patients. They also test for specific antibodies: anti-Scl-70 (linked to lung fibrosis), anti-centromere (linked to limited disease), and anti-RNA polymerase III (linked to rapid skin progression).


Comments (14)
Del Bourne
The part about the diagnostic odyssey is so true. It is heartbreaking how many patients are dismissed as just having 'poor circulation' when they first mention Raynaud's. Early detection of those antibodies really is the only way to get a head start on the lung issues before they become irreversible.
Srikanth Makineni
Raynauds is a huge red flag
Danielle Kelley
Of course they say it's an autoimmune glitch! They want you on those FDA-approved drugs that just line the pockets of big pharma while they ignore the environmental toxins actually causing the collagen to harden. Wake up people they aren't telling us the real cause of the fibrosis!
Rauf Ronald
Adding to the skin care section, don't sleep on the importance of keeping the skin hydrated from the inside out too. Using a humidifier in the bedroom can really help with that tight feeling in the morning. Keep fighting and stay positive everyone!
Brady Davis
Oh wow a 3.2 doctor average. Truly a pinnacle of medical efficiency right there. I'm sure the patients just love spending eighteen months playing a guessing game with their own organs. Absolutely stellar service.
Toby Sirois
I already know all this. The real issue is that most people don't understand that dietary changes are the only way to actually manage the inflammation. If you aren't cutting out processed sugars you're just wasting your time with those meds. It's basic science and it's sad that most doctors are too lazy to tell you.
Timothy Burroughs
just typical that the us is the only place mentioning these fancy centers of excellence while the rest of the world suffers in the dark we need to bring that american efficiency everywhere or just accept that the system is broken lol
Dhriti Chhabra
It is truly commendable that medical research is advancing toward targeted therapies. I believe that with continued cooperation between international research institutions, we shall find a more effective way to mitigate the suffering of those affected by this condition.
Christopher Cooper
The mention of adaptive devices is such a vital point for maintaining dignity and independence. I've seen some incredible 3D-printed modifications for kitchen utensils that specifically help those with sclerodactyly. It is truly inspiring to see how technology is bridging the gap for those with physical limitations. We should keep pushing for more open-source designs for these tools so they are accessible to everyone regardless of income!
Vivek Hattangadi
I totally agree with the point about the multidisciplinary team! It's so much easier to handle when you have a coordinator who makes sure the cardiologist and the pulmonologist are actually talking to each other. For anyone currently in that diagnostic odyssey, just keep pushing and don't settle for an answer that doesn't feel right. You've got this!
shelley wales
It's so important to remember that while the physical symptoms are daunting, the emotional toll of a slow-progressing disease is just as heavy. Please be kind to yourselves and remember that you are not alone in this journey. There are so many supportive communities out there ready to listen.
Rupert McKelvie
The progress in stem cell transplantation sounds like a real game-changer. Even a 50% improvement is a massive win in the long run. Things are definitely looking up for future patients.
Alexander Idle
Honestly the sheer audacity of the medical community to call it a 'diagnostic odyssey' as if it's some grand adventure and not just a nightmare of incompetence. It is simply appalling. I find it absolutely thrilling that we have to pay thousands of dollars just to find out our skin is turning into a rock. Truly a marvel of the modern age.
charles mcbride
I am very optimistic that the rise of telemedicine will finally give rural patients the specialized care they deserve. It is a noble effort to reduce those hospitalization rates through virtual access.